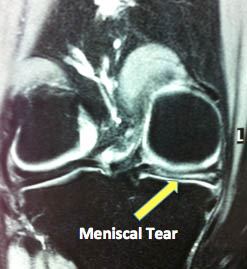
The meniscus (often incorrectly called the cartilage of the knee) is a soft rubbery structure between the femur (thigh bone) and tibia (shin bone). The knee has two compartments, the medial (inside) and lateral (outside) and each one has a meniscus which can be injured. Injury to the meniscus is very common (A Meniscal tear) and unfortunately almost always needs arthroscopic (keyhole) surgery to treat it.
Meniscal tears are broadly categorised into acute and degenerative tears. Many acute tears can be repaired to restore normal function to the knee but most degenerative tears are removed to relieve the pain they cause in the knee.
The meniscus acts as a shock absorber to protect the articular cartilage (joint lining cartilage) of the knee. The curved shape of the meniscus adds to the stability of the kof the kneesnee and helps with lubrication and nutrient transmission through the joint.
A knee which does not have a meniscus has a significantly higher chance of developing osteoarthritis in the long term. The severity and timing of this arthritis depends on many factors including your age, activity levels, weight and degree of meniscal damage.
On the whole when people talk about a cartilage tear, they are talking about a meniscus tear. When people talk about arthritis and wear of cartilage, they are usually referring to the articular cartilage on the ends of the bone.
Younger patients (and athletes) can usually recall a specific injury that caused their meniscus to tear. In older people the tear can occur with minimal or no trauma (such as standing from a chair). Tears can be simple or complex but the treatment cannot be decided on a MRI scan, it is always decided at the time of surgery when is can be carefully probed and checked for healing potential. The meniscus has a very poor blood supply and rarely heals without intervention.
Meniscal tears are almost always associated with a twist to the knee. Some people feel a pop and others a tearing sensation. Some people may just feel that “something is wrong” in the knee and the injury is not usually severe. Many people continue with sports or walk around without too much pain. There may be swelling of the knee but this is not always seen with an isolated meniscal tear.
The pain is usually localised to the side of the knee where the tear is located (medial or inside the knee is far more common than lateral or outside).
If the tear is acute (a bucket handle tear) there may be locking of the knee (when the knee gets stuck and can’t be moved). Sometimes a fragment of the meniscus gets stuck in between the bones and the knee can’t be straightened fully.
Giving way and clicking are not common with an isolated meniscal tear. Giving way is usually from the muscle relaxing when it is pain rather than the knee being unstable.
The diagnosis of a meniscal tear can usually be made based on the history and examination alone. In some situations I will arrange for you to have a MRI scan to exclude other injuries to the knee. This is usually not needed unless the diagnosis is in doubt and may delay treatment.

Initial treatment is the same as any acute injury. Rest and Ice the knee, keep it elevated and put a bandage or knee brace on if it makes you more comfortable. There is no urgency to be seen by me unless you have a locked knee (The meniscus can be damaged when it gets caught between the bones of the knee joint).
Unfortunately the meniscus rarely heals itself (due to its poor blood supply) and treatment for a meniscal tear usually involves an arthroscopy. The torn meniscus can be trimmed or repaired. The decision whether to repair or not is based mainly on the location and nature of the tear. Your age, activity levels, occupation and sporting demands are taken into account when making this decision. The final decision is made at the time of surgery as it depends on the size and site of the tear as well as the quality of the remaining meniscus.
Where possible I repair the meniscus using all arthroscopic (keyhole) techniques using specially designed endoscopic devices. There are times where traditional repairs techniques are needed which involve larger cuts around the knee.
The major advantage of meniscal repair is that it maintains the protective role of meniscus and reduces the chance of arthritis.
The major disadvantages are: that a longer rehabilitation period with longer restriction of work and sport activities; and that not all repairs heal (up to 20% of patients require a second keyhole operation to remove the broken fragments).
Overall if a meniscus can be repaired (in the right patient with the right type of tear) it is best to do so as it protects the knee from premature arthritis.