As a form of surgery, total knee replacement is one of the most cost effective and beneficial operations in modern society. The great majority of people are happy with their knee joint replacement and the outcome of their operation. There is a lot of information below but it is important to read it all so you can make an informed decision before you undergo knee replacement surgery. You must not proceed until you are confident that you understand this procedure and particularly the potential complications. A good knowledge of this operation will take away a lot of the stress you may have.
What Are The Benefits Of A Total Knee Replacement?
Living with pain for the rest of your life is a daunting prospect. Luckily for most people the arthritis pain can be relieved by having a total knee replacement operation. During the surgery your damaged knee joint is replaced with an artificial joint (a prosthesis or implant). After a total knee replacement you should be able to move more easily and without pain. Most people gain all the following benefits…
- Stops (or greatly reduces) arthritis knee pain.
- Improves quality of life – allows you to do your activities of daily living and low impact activities in greater comfort.
- Enables you to sleep without pain.
- Provides years of reliable knee function – Most total knee replacements last for many years
What Is A Total Knee Replacement?
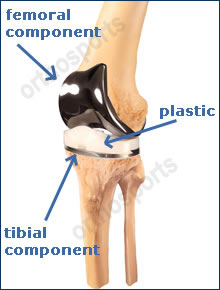
A knee replacement is quite literally removing the knee joint and replacing it with metal and a high grade medical plastic called polyethylene. The knee joint is made up of:
- the joint lining cartilage covering the end of the thigh bone (femur),
- the top of the shin bone (tibia)
- the knee cap and
- the joint lining capsule.
The damaged surfaces of the knee are removed and replaced with metal and polyethylene. The back surface of the kneecap (patella) is also commonly replaced. The implant or product used for the total knee replacement is referred to as a prosthesis. The knee replacement is typically fixed to the bone using a special bone cement (polymethylmethacrylate) but press fit or uncemented options are used in some situations. I will discuss this with you.
Total knee replacement began in the 1970’s as a treatment for painful and stiff knees. Since then arthroplasty (another word for knee replacement) has become a very common procedure for the treatment of arthritis.

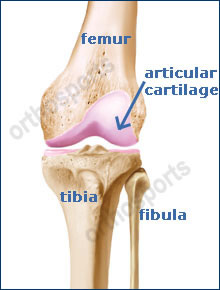
The knee joint consists of the femur, tibia and patella. The femur (thighbone) is the bone connecting the hip to the knee. The tibia (shinbone) connects the knee to the ankle. The patella or kneecap is the small bone in front of the knee. The fibula is a shorter and thinner bone running next to the tibia on its outside which has limited function. The knee joint acts like a hinge but with some rotation. The knee is connected by strong ligaments and surrounded by muscles. The ligaments of the knee joint stabilize the knee, allowing it to function normally. The cruciate ligaments (anterior and posterior) are important structures, which guide the knee in its normal motion. The joint lining cartilage (articular cartilage) is a smooth, friction free surface which coats the ends of the bones to create a joint. Any damage to this surface interferes with it’s normal functioning. Technically damage to this is called arthritis but the term is usually reserved for when the joint becomes stiff and painful.
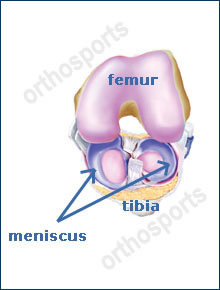
The structure that people often refer to as the cartilage of the knee is actually called the meniscus. This is a specialised structure between the femur and tibia and one is found between both sides of the knee (medial and lateral meniscus). These are the shock absorbers of the knee which help distribute load, stabilize the knee and aid in lubrication of the knee joint. Meniscal tears are often treated with arthroscopic (keyhole) surgery and any damage to the shock absorber allows arthritis to develop in the knee many years later.
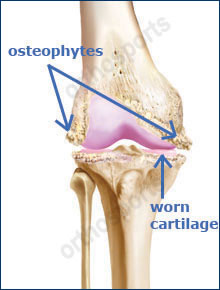

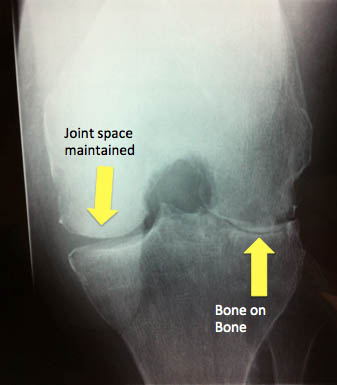
Pain in the knee can come from the bones or the soft tissue structures in the joint. Damage to the joint lining exposes the underlying bone and when the bones rub together pain is felt. The joint lining cartilage can be damaged rapidly in an accident or gradually wear away with time. As part of the natural process of ageing the cartilage starts to crack and wear away to expose the bone underneath it. Inflammation of the capsule and synovium of the joint can also cause pain in conditions like Rheumatoid arthritis. Pain is often experienced when the knee is damaged or inflamed and movement is often lost. Once the process has started it can never be stopped but the rate at which the deterioration takes place can be slowed.
No matter what age you are, a knee problem may keep you from activities you enjoy. Pain and stiffness may even limit your day-to-day activities. Problems with the knee joint tend to build up over time.
The most common cause of knee pain is osteoarthritis of the knee but any of the diagnoses listed below can cause enough problems to require a total knee replacement.
- Osteoarthritis

As time goes by, normal wear and tear can add up. Cartilage may begin to wear away (osteoarthritis). As the bones rub together they become rough and pitted. Damage to part of the meniscus (cartilage / shock absorber) and / or damage to the anterior cruciate ligament inevitably lead to osteoarthritis of the knee eventually.
- Inflammatory Arthritis
This is a group of conditions where the lining of the joint becomes inflamed (red and irritated) and releases a substance that destroys the joint lining (chondral) cartilage. In these conditions, more than one joint is usually affected. The joints are hot, swollen and painful and deformity is common. - Avascular Necrosis
Avascular necrosis is loss of blood supply to the bone. There is often not an obvious reason for this to happen (idiopathic) but it can be caused by a number of conditions or medications (such as long-term use of alcohol or steroids). If the bone dies (necrosis) then the joint will become arthritic. This pain often comes on quite suddenly without a specific injury and may increase rapidly. Avascular necrosis can happen at any age and while there are many other causes of this condition, the condition itself is rare. - Fracture
A bad fall or blow to the knee can break (fracture) a bone. If the broken bone does not heal straight the joint may slowly wear down like a tyre that is not well aligned. A fracture into the knee joint can lead to a rough joint lining surface which will make the opposing joint lining surface rough as well and eventually require treatment with a knee replacement. - Ligament injury
Injuries to ligaments can cause instability of the knee. Each time the knee gives way or dislocates it damages the joint lining. This can lead to premature arthritis if not corrected. - Childhood Knee Problems
Occasionally knee pain results from a problem, which may have started in childhood such as osteochondritis dissecans, trauma or juvenile rheumatoid arthritis.
Osgood Schlatters disease does not cause arthritis. - Infection
Infection can destroy the cartilage lining leading to osteoarthritis. - Other causes
Long term exposure to sports or heavy manual labour (unusual).
Other rare diseases affecting bones or soft tissues can also cause severe pain in the knee and may lead to arthritis.
- Inflammatory Arthritis
Arthritic Knee
How Do I Know If And When I Need A Total Knee Replacement?
It is usually quite clear to my patients when they are ready for a knee replacement. Typically they come to me and say “I can’t live like this any longer”. This is different for different people but usually means that you are having pain despite taking pain killers. Typically you will have trouble sleeping at night time, you will be able to walk a short distance and the pain is stopping you doing the tasks you wish to do. Some people experience pain that prevents them from being able to get up or down steps or they notice that their leg is becoming crooked (usually a bow legged deformity).
Non surgical treatment is continued for as long as possible before total knee replacement is considered. This includes pain killers, supplements, anti-inflammatory tablets, weight loss, injections and physiotherapy.
Total knee replacement is the end of the line for a knee that has advanced arthritis with painful grinding of the two bone ends. The decision whether or not to operate is not based on how bad the xrays look but rather on how much pain and disability you are experiencing.
Total Knee Replacement (TKR) Surgical Technique
The goal of knee replacement surgery is to give you back better function from your knee.
The anaesthetist will see you before the surgery. They will discuss with you the type of anaesthetic you will have. Typically a spinal anaesthetic is combined with sedation or a general anaesthetic. After you are taken to the operating theatre you will move on to the operating table and a tourniquet will be placed around your thigh. These days this is used for only a short period of time during the surgery.
A urinary catheter will be placed in your bladder to measure your fluid balance during and after surgery.
A cut (incision) is made in the skin on the front of the knee and continued through the underlying tissues to expose the knee joint.
Shaping the Distal Femoral Bone: Having moved the tissues safely out of the way the bone is addressed. Where possible I use a specially designed and customized cutting guide which “locks into place” in just the right spot on the bone. This device is used to make sure the bone is cut at exactly the right angle and rotation. If the knee arthritis has made the patient bowlegged or knock-kneed this is corrected during the operation. The custom cutting guide device is used to cut several pieces of bone from the end of the femur so the artificial knee can replace the worn surfaces with a metal surface.
Shaping the Tibia: The top of the shin bone is removed to allow a metal ‘tray’ to be inserted which can receive a plastic liner ‘locked into’ the top of it.
Replacing the Kneecap: The arthritic area of the kneecap is removed and replaced with a plastic lining.

- Trial components are put in first to make sure everything fits properly. Having confirmed a perfect fit of the implants the real components are then definitively inserted.
- The polyethylene spacer which was inserted can be replaced later if it wears out (prolonging the lifespan of the artificial joint).
- Drains are sometimes inserted.
- The wound is carefully closed.
- A dressing is applied and you are taken to the recovery room.
- Your leg will be bandaged from the groin to the toes.
- Your fluid input and output is measured carefully. A drip in the arm will be used to give you fluid and antibiotics and perhaps replacement blood after the operation if needed.
- Pain is normal after the operation but if your pain is not tolerable be sure to tell the nurse. Pain medication may be injected into a muscle or delivered through the drip into the blood stream.
- In some instances the anaesthetist will give you a device called Patient Controlled Analgesia (PCA) which allows you to control your own pain medication. When you push the button, pain medication is pumped into the drip. PCA pumps can provide a steady level of pain relief and have built in safety features which ensure you do not get too much medication.
- The drip, drains and catheter are removed at approximately 24 hours after surgery.
- Blood will be taken 24 to 48 hours after the operation to check your haemoglobin and blood chemicals.
- Your exercise regime will begin as soon as you are capable and this will continue during your stay in hospital and once you are at home. This will be supervised by a physiotherapist.
- You will be discharged approximately 5 days after the operation, depending on your progress. In most cases you will be sent to a rehabilitation center before you go home to have hydrotherapy and physiotherapy.
- You are in hospital approximately 5 days. At Day 2 you will get up on a frame and then you progress to crutches and then a stick usually by 4- 6 weeks.
- You usually go from hospital to rehabilitation and you are in rehabilitation for one to two weeks. This will include aggressive physiotherapy and hydrotherapy.
- When you leave hospital you will probably still require tablets for pain but no injections. Wean your medications down to panadol as soon as possible. Make sure you don’t stop exercising because you are in pain. It is better to use the pain killers and get the knee moving. The pain settles quite quickly so you are unlikely to be on the pain killers for more than a few weeks.
- Try to avoid taking anti-inflammatory tablets for one week after the surgery if you can.
- Typically you will lose 60 to 80 percent of your pain by six weeks and 95 percent of your pain by twelve weeks. By twelve weeks you can usually walk as far as you want to.
- Regaining movement early is extremely important. Keeping the knee fully straight is probably more important than bending it. Do not put anything under the knee even though it feels comfortable that way as this will make it much harder for you to get the knee straight in the long run. You must bend it as well and if you have not achieved enough bend yourself by about 3 months after the surgery then I may have to help you bend it with another anaesthetic and an overnight stay in hospital.
- Typically you will be well enough to return to work eight to twelve weeks after your operation. Heavy manual work may take longer. Normally by three months you can play sports like golf, bowls and ride a stationary bike ride but activities such as bush walking and doubles tennis can take a bit longer.
Any operation has risks. The following can occur with any surgery and some rarer complications may also be possible. It is impossible to discuss every complication and there will be some, which no surgeon may anticipate or may never have heard of. The utmost care is taken at all times during surgery to prevent these complications. I am a subspecialist surgeon and I believe this minimises the risk of complications.
The following list is not exhaustive and some are explained in more detail in other sections. Some are best discussed with an anaesthetist. Please let me know if you would like to speak with your anaesthetist prior to the day of your operation.
Infection
One of the risks after total knee replacement is infection. Infection may be superficial (i.e. in the skin) or deep (around the prosthesis). The risk is approximately 1%. If you do get an infection it will be treated aggressively with antibiotics but occasionally re-operation is necessary to clean out the infected material. In very rare circumstances, the knee replacement is removed and another one put in at a later time (six to eight weeks later when the infection has cleared up on drip antibiotics).
Fracture (breaking) of the Femur, Tibia or Patella
This may occur during surgery and may at times not be recognized. It may require more extensive surgery during the operation and very occasionally re-operation a few days later. The bone can also break around the implants if you fall heavily enough on the knee after the surgery.
Stiffness (lack of movement)
Some people form excessive scar tissue after their total knee replacement The average person will eventually bend their knee to 110 degrees after their total knee replacement. Some people achieve more than this but full range of motion is not possible due the shape of the prosthesis. A minimum of 90 degrees of flexion is required to be able to stand from a chair without using your hands to lift you up. If you are not bending past 90 degrees by twelve weeks after the surgery you may be readmitted to hospital for one night. Under epidural or spinal anaesthetic the knee is gently manipulated to break the internal scar tissue which is stopping you bending.
Damage to Nerves or Blood Vessels
During the operation, nerves or blood vessels may be damaged. These may be repaired at the time if recognized but may require a second operation to explore or repair any damage. It is very rare that a damaged nerve does not recover on its own. If a damaged nerve does not recover it can lead to poor function of the leg below the joint replacement such as a foot that does not work properly due to weakness or sensory loss.
Blood Clots
Blood clots can form in the calf muscles and they can travel to the lung. These can occasionally be serious and even life threatening. These blood clots will be treated immediately and every measure is taken to avoid these occurring. You will be given a blood thinning agent by injection during your stay in hospital. Stockings will be provided for you which aid in trying to prevent blood pooling in the veins in the calf and you should wear these for six weeks after the surgery. A mechanical device is also used during the operation on the non operated leg to encourage blood flow. You should take one aspirin per day for 3 months (unless it is contraindicated in you) to thin the blood after you leave hospital.
Wound Irritation or Breakdown
Cutting the skin always cuts some skin nerves so you will have a patch of numbness around the wound. This does not affect the function of your joint but may be disconcerting for you over the short to medium term. Eventually the numb feeling improves and does not worry most people. Occasionally, instead of a numb sensation you will have burning or a hypersensitive sensation in the wound. This usually settles down over many months but occasionally can be long term and troublesome. Occasionally there is some aching around the scar for many months, which can become worse in cold weather but this usually is nowhere near as uncomfortable as the pain you had before the operation.
Wound breakdown is rare but if it does occur it may require surgery to repair it. You can also get a reaction to the stitches used if your body does not dissolve the material the way most people do. This usually appears as a small pimple on your scar and pulling the bit of thread out with some tweezers and applying an antiseptic dressing is usually all that is required. Occasionally a short course of antibiotics is required.
Wear
The ‘weak link’ of total knee replacement is the plastic liner. It is needed to stop the metal surfaces rubbing on each other. It is designed to wear out very slowly just like the tyres on your car. The harder you are on the joint, the faster it will wear out. I don’t recommend people return to heavy manual labor or play pounding sports like jogging or soccer after the surgery. Normal walking is not a problem for the joint.
Most knee replacements have about an 85 to 95% percent fifteen year survival (are still working well 15 years after they are inserted). There are a large number of factors, which affect the survival rate. Continual improvements in technology make these components more likely to last for a longer period of time.
If there is significant wear in the joint then the liner may need to be replaced. Wear can sometimes causes loosening of the metal from the bone and the whole joint may then need replacing. This is why we suggest that you have xrays performed of the knee every fews years for the rest of your life. We assess your x-ray to make sure that nothing worrying is occurring in the knee joint before you get symptoms. It is extremely important that you do not lose contact with a surgeon during the life of your knee replacement and if you move away from Sydney please talk to me about finding another surgeon to look after you.
Osteolysis
This means part of the bone is reabsorbed or disappears. This is a result of small wear particles setting up a reaction in the body causing the bodies normal cells to attack the bone. Occasionally I may recommend you have a procedure to change the liner (bearing surface) or bone graft these defects before they become major problems.
Damage to Ligaments
There are ligaments (collaterals, quadriceps, patella) surrounding the knee, which can be damaged before or after surgery. Damage to these ligaments can cause instability of the knee or the inability to straighten the knee. Depending on the circumstances this may require a brace or further surgery.
Heterotopic Ossification
This means bone forms in the soft tissues surrounding the knee. This can cause discomfort and stiffness and occasionally needs to be excised. This is quite rare in the knee.
Cosmetic Appearance
The knee may be more swollen than the other one or it may be a different shape then prior to surgery. This is normal as I place the knee in its proper alignment during surgery. It looks different because it was an abnormal shape because of the arthritis. The scar might be unsightly or thickened.
Breakage of the Implant
This is very rare and requires more surgery to remove the broken implant and replace it with a new one.
Neuroma Formation
This is an irritation of a superficial nerve resulting in pain, tingling and hypersensitivity around the scar area.
Complex Regional Pain Syndrome
This is an unexplained condition where nerves become hyperactive and the limb painful. This may occur following minor trauma or surgery. This usually but not always resolves over time but may require referral to a specialised pain clinic.
Pressure
Pressure on areas of the body in the operating theatre causing nerve damage.
Diathermy Burns
Diathermy burns from cautery device used in most open operations (very rare).
Failure to Relieve Pain
This is not common but unfortunately, some operations may not be entirely successful in relieving pain.
Limp
Limp can occur from muscle weakness.
Bed Sores
Bed sores occur from pressure areas on the skin during bed rest.
Other
Any medical complication you have heard about can occur especially if you already have a pre-existing medical problem. Such complications include heart attack, stroke, kidney failure, pneumonia, bowel obstruction, bladder infection or obstruction etc. Serious medical problems can lead to ongoing health concerns, prolonged hospitalisation or rarely death.
Results
Total knee replacement surgery is generally very successful. It is an excellent procedure to improve a person’s quality of life. After this operation 95 percent of people are good or excellent. ‘Good’ means occasional aches and pains which do not require painkillers and ‘excellent’ means no significant pain or discomfort. There are some people who will have unexplained pain.
In general, 90 –95% of knee replacements survive 15 years but this depends on a number of variables such as your age and activity level. I think of the new joint as I would a tyre on my car. The more you drive on it the quicker it wears out. The better it is looked after the longer it will last.
- Remember this is an artificial knee and must be treated with care.
- In general, the more active you are the quicker your knee will wear out.
- You can drive when you have regained muscle control, usually by 6-12 weeks.
- Avoid situations where you might fall.
- Your knee may go off in a metal detector at the airport.
- Prevention of infection is vital. If you have any infections anywhere make sure you see your local doctor straight away for treatment. If you get increasing pain in your joint and are sick and have temperatures you should go to hospital or see me immediately.
- USE OF ANTIBIOTICS – Antibiotics should be prescribed if you have an infection anywhere in the body. There is mixed evidence as to whether antibiotics are required if you have surgery in ‘dirty’ areas such as your mouth, nose, bowel, bladder, feet or urinary catheterization. Feel free to discuss this with me in more detail.
Activities
- You should avoid pounding activities, which put a lot of stress on the joint.
- Walking is good.
- Swimming in a pool or light surf between the flags is safe.
- Doubles tennis is allowable but anything more aggressive will lead to premature wear of your joint. Contact sports are forbidden and jogging can be detrimental to the long term survival of your joint replacement.
- Skiing on groomed slopes if you are a good skier is acceptable as long as you are aware you can cause significant damage if you fall.
- Bowls and golf should not be a problem.
Although every effort has been made to explain the potential complications there will be complications that may not have been specifically mentioned. This is because they are relatively rare. Feel free to access other sources of information from the Internet, other patients and your local doctor.