



Most people only stay in hospital for one or two nights. You are seen by a physiotherapist who will teach you exercises which must be performed 3-4 times per day. The specific exercises will vary depending on the location of your cartilage defect. Most people commence immediate motion of the knee and are allowed to put some weight through the leg (partial weight bearing) for 6 weeks and then increase to full weight bearing by 12 weeks. This again depends on the location of the articular cartilage injury.
The cartilage takes 12 – 18 months to mature fully so patients typically do not return to load bearing exercises before the 12 month mark. Non loading bearing exercises such as swimming and cycling are started much earlier.
This operation is usually done to relieve pain and swelling on a day to day basis rather than to return people to high level sport.
You may need to wear a knee brace to limit the amount you can bend your knee after the operation. A graduated exercise programme will be given to you but will vary from patient to patient. A general guide for postoperative care is listed below.
This operation is not designed to get you back to sport. It is to prevent the onset and progression of arthritis in your knee. Returning to sporting activities should be considered a bonus (if it is possible) rather than an expected outcome of the surgery. As a general rule it is not possible to return to sports involving running and twisting for 12 months.
The time taken to return to work will depend on what work you do. If you sit at a desk all day and can be driven to and from work then you will probably be able to return to work on crutches at 10-14 days after the chondral grafting operation. Recovery from a high tibial osteotomy is slower and usually associated with more pain. Physical jobs, particularly those involving walking and lifting, may take 6 months or longer.
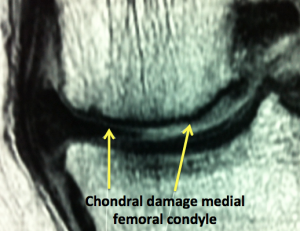
Rehabilitation varies greatly between patients as it depends on the size and site of the lesion. No two knees are exactly the same. The amount of weight you will allowed to take on the leg and the amount of bend you are allowed will depend on the location of the chondral lesion seen at surgery. If the damaged area in in a part of the knee which does not take load when you are walking then the whole process can be accelerated.
Week 1
- Allow wound healing
- Weight bearing – nil
- Motion – nil or slight flexion except if on CPM machine
- Brace – locked as appropriate
- Ambulation – crutches
- Physio – rest
Week 2-6
- Weight bearing – none to partial
- Motion – passive up to 90 degrees
- Brace – limited flexion
- Ambulation – crutches usually non weight bearing
- Physio – reduce swelling, closed chain, isometric quads, gentle cycling, walking or treading water in a pool
Week 6-12
- Weight bearing – progress to full
- Motion – progress to full
- Brace – discard
- Ambulation – wean off crutches
- Physio – open chain, proprioceptive exercises, resisted cycling, swimming avoiding breaststroke
Week 12-52
- Gradual increase in all exercises to strengthen quads and hamstring muscles, jogging at 6 months, sport by 12 months
This procedure has good results for localised articular cartilage lesions. Without treatment a lot of these lesions progress to arthritis. It does involve a lot of rehabilitation and commitment to physiotherapy but once this is over the majority of patients are happy with their outcome.